With the early onset of immunohistochemistry (IHC) in the anatomic pathology laboratory in the early to mid-1980’s, it soon proved to be a useful tool in a number of different areas of specialty including dermatology. Particularly in sun-rich states such as California, Florida, Arizona, and Texas, there was a high prevalence of skin cancers. Dermatopathologists commonly used the routine Hematoxylin & Eosin (H&E) and a few select special stains to determine the morphology of skin diseases. These were done using a standard positive tissue control slide stained side-by-side with the patient case slide. Immunohistochemistry allowed them to effectively differentiate between melanoma, sarcoma, and carcinoma. While squamous cell carcinoma is the second most common form of skin cancer, melanoma has the potential to rapidly metastasize to other organs. This diagnostic differentiation was critical and quite often required multiple IHC stains to be performed, thus the need for a panel of stains. IHC staining initially followed this same pattern of patient slide stained side-by-side with the positive antibody control slide.
One of the early basic screening panels in dermatopathology for the aforementioned disease states was S-100, Vimentin, and Cyto-keratin. This would be used to differentiate between melanoma, sarcoma, and carcinoma looking for strongly positive, moderate, or negative expression of the antibodies in tissue. Specificity in diagnosis was vitally important in prognosis and treatment. In 1988 a small company titled ‘Southern California Immunoperoxidase Services’ developed a Multi-Tissue Control block for its dermatology accounts with three tissues representing positive staining for each antibody. This aided dermatopathologists by allowing them to review the expected staining patterns in the control specimen much more efficiently without having to repeatedly change slides for each antibody. It also strengthened their quality assurance by ensuring that all three tissues were handled the same.
Initially there were no instruments, devices, or aids in creating a Multi-Tissue Control for not only IHC but other histological stains also. This procedure was totally manual and required thought in tissue selection and the careful skill of the Histologist in separating the desired tissue pieces and forming them together in a communal block. For the most part known positive tissue pieces were identified from existing control or archived patient case blocks.
They were then melted down from the various donor blocks and reassembled into a communal block.
With the popularity of Multi-Tissue Control blocks being used, tools were created to facilitate ‘punch’ biopsy tissue sections taking small represenative pieces from a donor block (left image), and inserting them into a new recipient control block (right image). The method was still simple and allowed the technologist to create a control block and custom design it to represent a specific staining panel for special stains or immunohistochemistry.
Continued development in the sensitivity of antibodies created a whole new array of markers for dermatopathologists to choose. HMB45, MIB-1 and a host of others gave a greater diagnostic specificity for melanoma in many cases than the more general staining of Vimentin. AE1/AE3 and Bcl-2 gave greater sensitivity to squamous cell and basal cell carcinoma respectively. Further advances in antibody development led to a greater need for expanded panels. This diagnostic need ultimately led to the development of Tissue Microarrays (TMA) which provided a wide spectrum on staining patterns and intensity in various tissue types. This was and still proves to be the ultimate in staining panels particularly in research, however, in smaller lab systems set up for a more clinical (hospital-type) application, the simple Multi-Tissue Control block is more appropriate and cost effective.
As in any quality control measure that is developed, Multi-Tissue Control blocks must be created with a tested and validated procedure that includes tissue acquisition, and a protocol for communal block assembly, testing/staining, technical review, sign off, and documention. Developing your own Multi-Tissue Control block still satisfies the existing need from the early days of development. It provides a custom-designed panel of stains specific to the needs and interest of the Pathologist and helps in making their job of diagnoses more streamlined and efficient. While this diagnostic tool can be purchased from commercial vendors, creating your own MTC block gives a certain personal gratification and greater confidence in your quality assurance staining system.
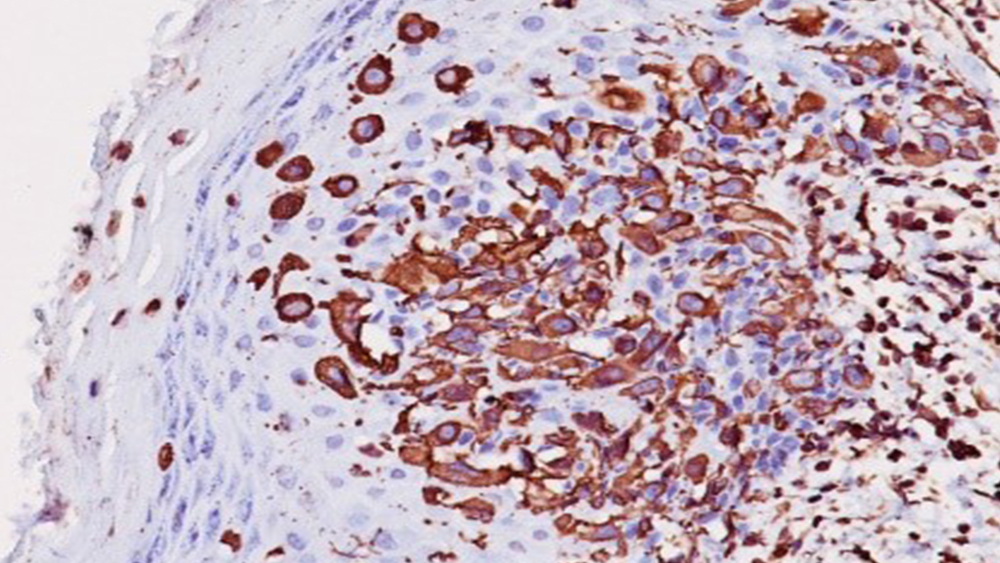
Cutaneous melanoma stained with Vimentin Ab (left);
Basal cell carcinoma stained with Cyto-keratin Ab (right)
References:
1. Brown, S., ‘Developing & Validating Multi-Tissue Control Blocks’, Workshop in Technical Development Series, Lab Management Consultants, 2020.
2. Labstore.com, T-Sue Technology.
3. ResearchGate.net, ‘Basal cell carcinoma staining’.
4. SCBT.com, ‘Cutaneous melanoma staining’.
Early Development of Multi-Tissue Control Panels for Diagnostic Dermatopathology