End Stage Renal Disease (ESRD) can be defined as a condition of renal function that has digressed to the point that the kidney no longer performs at a level that is self or even life sustaining. When this happens some form of life sustaining intervention must be employed to compensate for the kidney’s blood cleansing/regulation process that is severely compromised or no longer existent in the host kidney. Recent estimates reveal that the prevalence of End Stage Renal Disease is over 750,000 per year in the U.S. International estimates show that 2 million people worldwide suffer from ESRD with the numbers increasing by 5-7% each year. The two primary methods of clinical treatment of ESRD are renal dialysis and/or kidney transplant, however, diagnoses must be made to first determine that the patient has ESRD, and secondly what specific type of disease exists.
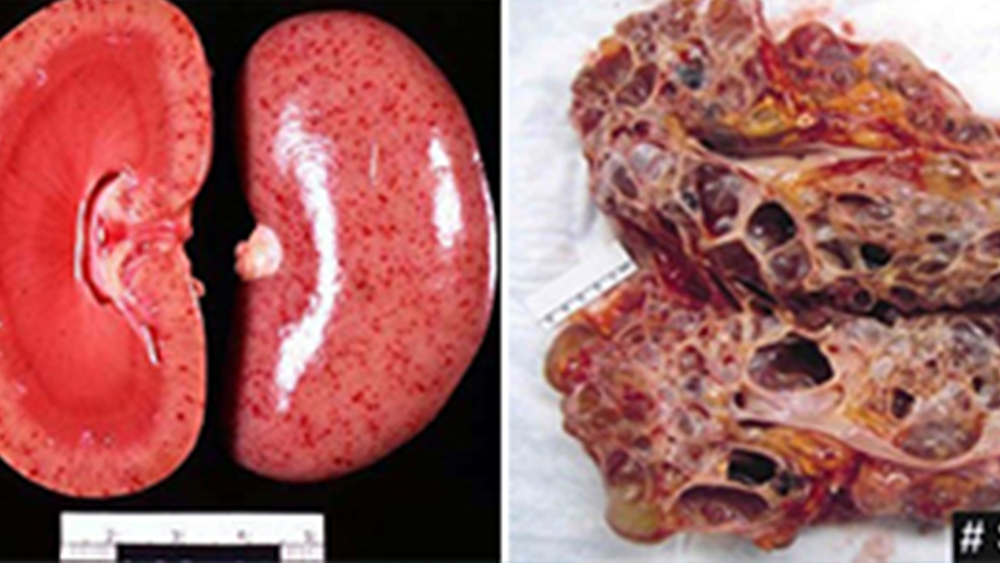
Blood chemistry levels are typically the first sign that renal function is compromised, but Histopathology is the primary methods used to visualize the anatomic pathology and thus isolate the specific condition. The images to the right illustrate two bisected kidney specimens. The one on the left demonstrates the smooth normal surface and interior of a normal kidney. The image on the right is the gross

pathology bisection of a kidney with Polycystic Kidney Disease (PKD), a chronic kidney disease leading to ESRD. Note the large cystic structures that have taken over most of the normal parenchyma. As revealing as the gross pathology shows, it is the Histoechnologist that the Pathologists truly depend on to give him the morphologic cellular imagery that he needs to understand the pathology and its manifestation into normal tissue. Renal histopathology is one of the areas that the skill and accuracy of the Histotechnologist is most revealed, as typically the micro-sectioning of this tissue is at the 2-4 micron levels requiring extreme focus, flawless technique, and precision equipment. The Pathologist needs to see a 1-2 cell layer
resolution of the tissue because delicate structures such as the glomerular tufts, which are the kidney’s key component in filtering and cleansing the blood system, give one of the best keys to solving the mystery of exact diagnoses. The above left image is a normal glomerulus sitting within its Bowman’s Capsule, visualized using a PAS-H special stain. Blood enters and

exits in the lower part of the tuft, and is filtered through the tiny delicate glomerular tubules in between. On the right we see a glomeruli in a polycystic kidney. Note how the cystic fluid has filled and expanded the Bowman’s Capsule, and severely compromised the glomeruli to be squeezed into the upper left section of the capsule. The fluid pressure from the cyst has significantly reduced its ability to filter blood and all but detached the glomeruli from the capsule wall. To be able to show a representaion of a micro thin, 2-cell layer section of the renal cystic tissue, all while sectioning delicately enough to maintain the fluid layer in the cyst with its relation to other structures and tissue stroma; again this takes exceptional skill in microtomy.
Routine Histopathology is only one method for renal pathology investigation used by the Histologist. Other more advanced methods such as special stains, immunofluorescence, etc., give an even clearer picture of the disease and how it has progressed. These images created by the Histologist give the Pathologist the evidence needed to determine exactly how an ESRD condition is compromising the renal performance. Electron microscopy was employed in the image to the right and demonstrates a thickening of the capsule (Bowman’s) wall. This thickening causes further disease progression and compromised function. The image below is a glomeruli section stained with immunofluorescence methods. The positive staining illustrated in the green fluorescent reaction is indicative of strong granular peripheral and mesangial staining for C3 antibody, and a moderate focal staining for fibrin antibody. This kind of data is critical in determining the extent of abnormal pathology and what treatment options would be best to improve renal function enough to be self sustaining, or move towards kidney removal and/or transplant.

These advanced methods and procedures require advance education, training, and oftentimes specialized equipment. Methods such as electron microscopy, plastic embedding, immunohistochemistry and immunofluorescent technique, go far beyond routine histopathology in transitioning from an image of structure and morphology to advanced detection at the antibody level, long before the abnormal tissue changes are able to be detected. Histotechnologists provide the tools the Pathologist needs to pre-screen patients for the probability of disease long before the disease manifests into tumor or begins to compromise health. Understanding this, we also understand that there is a responsibility for those in histopathology who are truly committed to diagnostic patient care; those professionals must always strive to learn, grow, and further develop themselves beyond the common worker. Advances in the medical profession are continually giving us greater tools (methods/procedures/instrumentation) to further unlock the mysteries of disease, and it is imperative that we, the Histology professional, continue to grow and advance with medicine to master those tools.
Whether it is routine histology or advanced, the intervention of the science and application of Histopathology in renal and other disease states has been the validating element confirming disease and further teaching us about the human body. Commendations to all Histopathology professionals. You drive the science that brings light and revelation to disease.
References:
- Centers for Disease Control & Prevention, http://www.cdc.gov/ckd.
- University of San Francisco, Kidney Statistics, https://pharm.ucsf.edu/kidney/need/statistics.
- Brown, S., “Case Studies in Diagnostic Renal Histopathology”, Lab Management Consultants, 2012.